


Vaccinated vs. Unvaccinated Deaths
According to UK data (the best)

The UK is generally considered to have the best data tracking deaths of Covid vaccinated and unvaccinated persons. I am drawing data here from “Deaths occurring between 1 January 2021 and 31 May 2022 edition of this dataset” found at “Deaths by vaccination status, England”.
Edit 28 November 2022: Prof. Norman Fenton has written about a problem with the British data, namely, that within a window of approximately 14 days of genetic injections, an injected person may be classified as “unvaccinated.” I did not account for this issue, as there was no way of doing so; but in any event, the resulting bias would be to increase vaccinated deaths. Denmark stopped recommending the genetic injections for persons under 50 on the basis of the same or similar data.
The data is broken down by age group as follows:
Unvaccinated
First dose, less than 21 days ago
First dose, at least 21 days ago
Second dose, less than 21 days ago
Second dose, between 21 days and 6 months ago
Second dose, at least 6 months ago
Third dose or booster, less than 21 days ago
Third dose or booster, at least 21 days ago
For each category, vaccinated or unvaccinated, the person-years accounted for are given. A person-year is one person for one year; two person years might be two persons for one year or one person for two years. This measure gives us a reasonable basis for normalizing death rates against life years. Others (“The Expose”) have done similar analyses, but I wanted to see for myself.
Because it is known via FOIA that the treatment arms of both Pfizer and Moderna six-month clinical trials generated more all-cause mortality than the control arms, only all-cause mortality is considered. The spike protein is nasty. It can induce a wide range of ailments, most of which were actually in the unpublished insert (per the FDA presentation) for the vaccines.
Since the temporal categories induce possible survivorship bias, caution needs to be applied to the results. Persons dying from a first or second injection won’t be around in the pool that gets the third one, for example. The data provided does not really give us a way to fix this that I can detect.
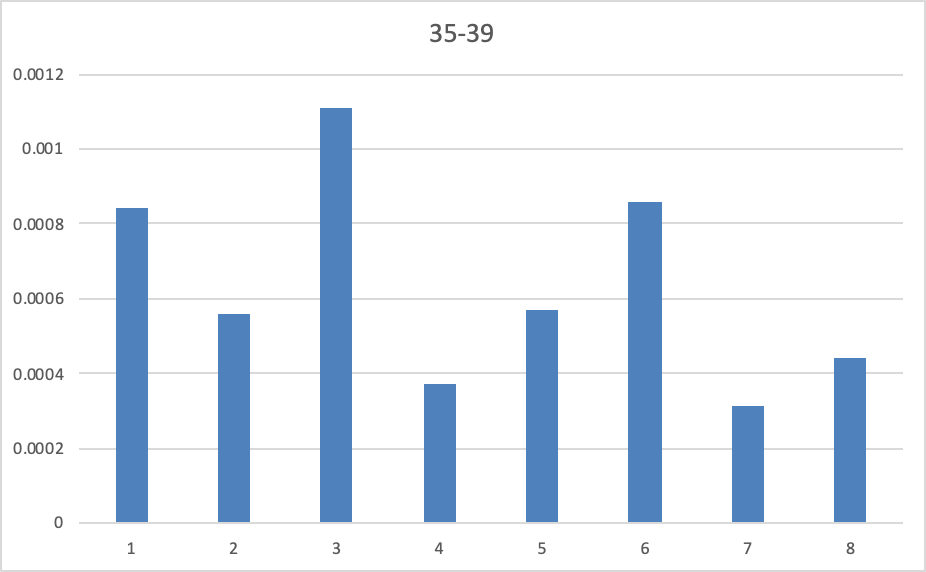
To calculate normalized death rates I simply divided the count of all-cause deaths in a category by person-years in the category. The result is on the y-axis; the injections are on the x-axis by number as given above.
The results vary by age group. As a practical matter, I assume that exposing oneself to greater risk than unvaccinated risk at any point in the sequence of doses and boosters is not to be desired.
Children and adults under 50 do not seem to benefit from vaccination. Following are the results by age group.
For 10-14, the salient result is the increased risk 6 months after second dose (6) for the youngest age group. There would seem to be no benefit to vaccinating this age group.

For 15-19 the risk concentrates at 6 months or more after second dose, with no clear benefit to vaccination.

For 2-24, risk peaked at first dose at least 21 days ago, with no clear benefit to vaccination.

For 25-29, risk climbs above unvaccinated risk 21 days after first dose, with no clear benefit to vaccination.

For 30-34, risk climbs above unvaccinated risk 21 days after first dose, with no clear benefit to vaccination.

For 35-39, risk climbs above unvaccinated risk 21 days after first dose, with no clear benefit to vaccination.
For 40-44, risk climbs above unvaccinated risk 21 days after first dose, with no clear benefit to vaccination; with a second peak at six months or more after second dose.

For 45-49, it looks like a crap shoot out to six months after second dose, with no clear benefit to vaccination.

For 50-54, one or two doses seem to confer benefit.

For 55-59, one or two doses seem to confer benefit.

For 60-64, one or two doses seem to confer benefit.

For 65-69, one or two doses seem to confer benefit.

For 70-74, one or two doses seem to confer benefit.

For 75-79, one or two doses seem to confer benefit.

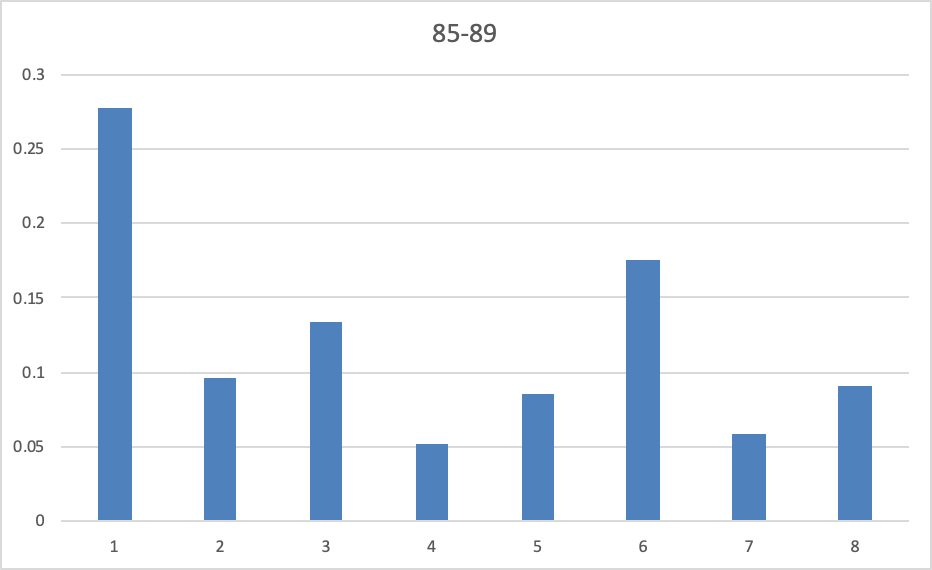
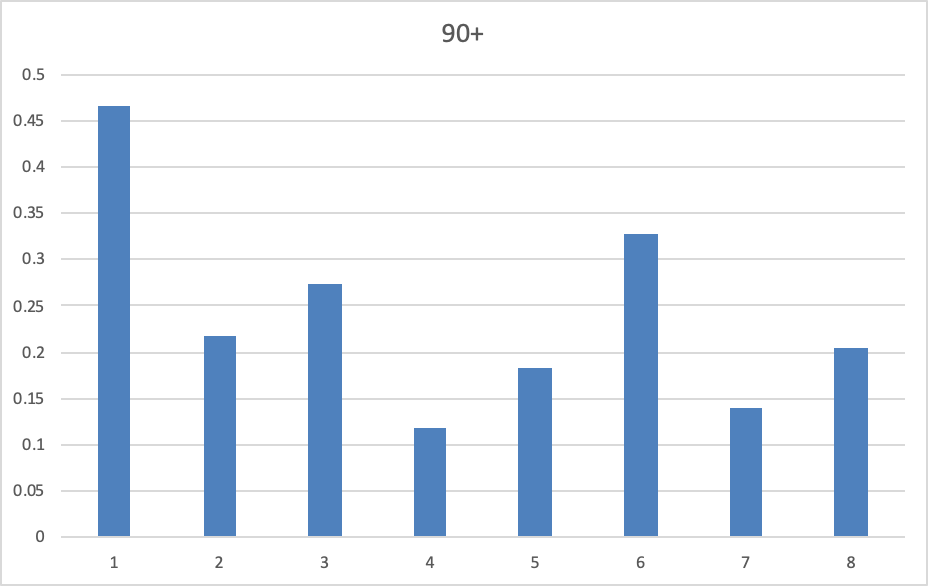
For 80-90+, one, two or three doses seem to confer benefit, although the survivorship bias may be particularly relevant here.

Disclaimer (added July 9, 2022): This post in no way is meant to recommend the mRNA injections, as there appear to be other risks associated with bio-distribution of the spike protein to organs throughout the body. This post is meant to point out that mass vaccination is not justified by the data so far, especially not to children.
I don't even think you need to provide any data on vaccine injuries or deaths to those under the age of, say, 30. Just accurately and properly report the risks of dying "from" Covid in these age categories.
I've written about one comprehensive study in the UK where researchers looked at deaths from Covid in the first year of the pandemic among UK children (0 to 17). If you take out the few deaths from children who had severe or "life-altering" illnesses, only six "healthy" children died from Covid in the first 12 months of the pandemic. There are approximately 12 million children in the UK, maybe 11.75 million who do not have "life-altering" medical conditions. This means the odds a "healthy" UK child would die "from" Covid are about 6-in-11.75 million (or a little less than 1-in-2 million mortality risk).
Do we really need to vaccinate approximately 11 million kids to (maybe) prevent one or two of these six deaths?
The odds a random person will get struck by lightning in a given year in the U.S. are about 1-in-700,000. So a random citizen's odds of getting struck by lighting are almost three times greater than the probability a healthy child will die from Covid in the same year.
We're vaccinating healthy kids who literally have a 0.000 percent chance of dying from Covid. You have to go out to FOUR decimal points to pick up the mortality "risk."